|
|
South West Public Health Observatory |
|
| The impact of drug misuse on health in the South West, 1996-2001 | ||
|
|
Drug use and problem drug misuseDefining the nature and scale of drug use is a complex issue. The British Crime Survey in 1998 revealed one third of adults (aged 16–59 years) in the UK had used illicit drugs, rising to half of 16–24 year-olds; thus the extent of drug use had increased in young people. 1 Of the 16–24 year age group, 30% reported taking drugs in the previous year and 20% in the previous month, with little difference between males and females. Results from a survey in 1998 on Smoking, drinking and drug use among young teenagers 2 showed 11% of 11–15 year-olds in England had used drugs in the last year, 7% in the last month.
In the South West, a survey in Bath and North East Somerset in 1999 3 reported 24% of 11 to 19 year-olds had used an illegal drug at some point, with cannabis being the substance most commonly taken (22%). The use of other drugs was significantly less widespread; 3% had taken solvents, amphetamines, poppers or magic mushrooms; fewer than 2% had taken cocaine/crack or ecstasy, and less than 1% had taken LSD, tranquillisers, anabolic steroids, ketamine, or heroin/methadone. Fewer than 2% of 11 year-olds had tried any illegal drug, but the prevalence of illegal drug usage increased rapidly amongst the older age groups. These findings are similar to other surveys, a useful list of which is available from the Office of National Statistics. 4
Whilst these results give cause for concern regarding the widespread nature of drug use in the young, raising issues about prevention and health promotion, without long term follow up it is difficult to gauge the prevalence of problems arising from them.
A recent report from the Health Advisory Service 5 on young persons’ needs recognises the difficulties in drawing clear distinctions between drug use and drug misuse. Whether regular or continuous use necessarily leads to drug dependency and problems is difficult to assess, as is determining the nature of progression from one drug to another. Those using cannabis may not graduate to drugs such as heroin or crack-cocaine, which create strong physical dependency. Moreover drug dependency is not just restricted to those using heroin or crack-cocaine, as there are people who are psychologically dependent on cannabis, but use no other drugs.
Attempting to discern incidence and prevalence of drug use, by the types of drugs, or by quantity and frequency of consumption, does not provide clear information to assist in planning and providing specialised drug services; estimates of the incidence and prevalence of drug misuse related problems and needs are required. Distinguishing between drug use and problem drug misuse, as far as our report is concerned, is made on a pragmatic basis, i.e. 'the consumption of drugs which affect thinking and feeling in a way which gives rise to legal, social, personal, health or financial problems for the user' . This is the definition applied by the Regional Drug Misuse Databases, and is quoted from the notification forms which health, social services, police, probation and prison services are requested to complete when in contact with an individual with drug problems.
Back
Scale of problem drug misuse
The 1990s saw a substantial increase in illegal drug taking throughout the country, not only in the use of cannabis and MDMA (ecstasy), but Class A drugs such as heroin, cocaine and crack-cocaine. Bulletins from the Regional Drug Misuse Databases (RDMDs) 6 have indicated annual increases since 1993 in the numbers of people with drug misuse problems notified by drug agencies in England, with 33,100 persons in the six months to September 2000 (compared to around 17,000 for the same period in 1993). A recent census by the RDMDs, of the numbers in treatment in England, reported 118,500 during 2000/01. 7 It should be clear that the national figures combine new cases with longer term repeating cases, such that the increases are cumulative and not representative of annual incidence.
The census found that 95% of the cases were between the ages of 15 and 44 years, 50% were in their twenties and 14% were under 20 years of age. The ratio of males to females was approximately 3:1.
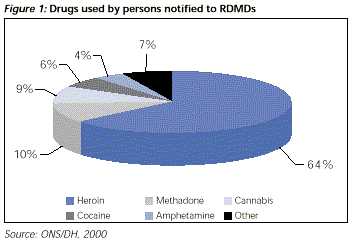
Figure 1 shows heroin was the most frequently reported main drug used (64%), followed by methadone (10%), cannabis (9%), cocaine (6%) and amphetamines (4%). Over half (54%) were recorded as using more than one drug.
Despite the risks associated with injecting drug use, of infection, overdose or death, 66% had injected, 45% within the four weeks prior to contact with an agency. Men (47%) were more likely than women (40%) to have injected, though women (25%) were more likely than men (20%) to have shared injecting equipment. Of those who shared, 21% had done so in the preceding four weeks.
By no means all persons with drug misuse problems are known to statutory agencies or notified to the Regional Drug Misuse Databases. A report by Drugscope, UK Drug Situation 2000 8 , estimated as many as 266,000 people with drug misuse problems in the UK. Attempts to determine the extent of hidden problem drug misuse have mainly focused on capture-recapture methodology (see Hay 9 for review). Briefly, this method estimates prevalence by examining the numbers of people with problems related to drug misuse, who are known to various agencies, making calculations based on the overlaps between them. Various other methods have been used, some of which are compared in a recent paper by Frischer and Hickman 10 and two of which we have used alongside a capture-recapture method, to estimate hidden prevalence in the South West.
Back
Government policy
Since the publication of Tackling Drugs to Build a Better Britain 11 in 1998 there have been several important developments concerning the implementation of government policy. Drug Action Teams (DATs) have been established at local authority level, with representatives of the main authorities involved as stakeholders. Partnership arrangements are being worked out involving health, social and probation services, voluntary organisations, education, the police and others. Inter-agency working and co-operation are seen as fundamental for a holistic approach to the formulation of local plans to meet the White Paper's objectives. The Second National Plan 12 has specified key performance targets for each objective, as follows:
Young people
Reduce the proportion of under 25 year-olds reporting the use of illegal drugs in the last month and year. Substantially reduce the proportion of young people using drugs which cause the greatest harm, heroin and cocaine by 25% by 2005 and by 50% by 2008.Communities
Reduce levels of repeat offending amongst drug misusing offenders by 25% by 2005 and by 50% by 2008.Treatment
To increase participation of problem drug misusers, including prisoners, in drug treatment programmes which have a positive impact on crime, by 66% by 2005 and by 100% by 2008.Availability
To reduce access to all drugs amongst young people… particularly heroin and cocaine, by 25% by 2002 and by 50% by 2008.Further targets were stated regarding prisons and drug trafficking. Arrest Referral Schemes, Drug Treatment and Testing Orders (DTTOs), together with mandatory drug testing in prisons reinforce the objective of getting offenders into treatment.
The National Treatment Outcome Research Study (NTORS) 13 has reported positive benefits from a range of treatment programmes in helping problem drug users to stop, and maintain their progress. A Home Office study in 1998 14 indicated approximately 60% of all crimes were drug related. The emphasis on treatment for prisoners is seen as providing an antidote to drug related crime. The establishment of the National Treatment Agency (NTA) 15 will set standards for a range of treatment efforts. Guidelines for auditing services have been published by the Standing Conference on Drug Abuse (SCODA) 16 and many areas already have systems for monitoring the quality of drug services, including the South West.
Back
Services for problem drug misuse
A mixture of statutory, voluntary and private agencies provides drug services. Most drug advisory services, needle exchanges and residential rehabilitation facilities are run by the voluntary or private sector, albeit with joint health and social services monies. The NHS varies considerably in the range of services it provides, with relatively few dedicated drug service beds. Detoxification and rehabilitation may take place in general psychiatry beds, or in the community under the supervision of Community Drug Teams (which in some areas may be combined with alcohol services) and, increasingly, in prisons.
Clinical guidelines for doctors were published in 1998 17 laying emphasis upon shared care arrangements. Based upon the right of drug users and their families to receive health care the same as any other citizen, general practitioners (GPs) have a key role in the identification, assessment and treatment of drug problems. Together with local specialised agencies the focus of the management of drug misuse problems is within the local community, with resources targeted towards local need.
Whilst the main responsibility for prevention, health promotion and substitute prescribing lies with the primary care sector and community drug teams, other health services and the hospital sector are engaged in providing a range of interventions concerned with the sequelae of drug taking, which are described below.
Back
Health effects on drug users
Deaths
Reducing drug-related deaths is a government priority and the subject of an important report by the Advisory Council on the Misuse of Drugs. 18 Fatal overdoses are the most common cause of death, resulting from cardiac arrest or respiratory failure. Abstinent drug users and those who have been drug free in prison, who relapse, are particularly at risk owing to a decreased dosage tolerance. 19 Deaths may also be a consequence of infection from sharing injecting equipment, overdoses with suicidal intent, or accidents and injuries. Drug related deaths have been increasing through the 1990s and are being monitored nationally by the Office of National Statistics and St. George's Hospital. 20,21,22
Infectious diseases
The spread of HIV/AIDS abated during the 1990s, with the number of new cases of infection amongst injecting drug users (IDUs) falling from 447 in 1986 to 99 in 1999. 23 Although this decline in the drug using population has been attributed to the swift introduction of needle exchanges, the prevalence of sharing injecting equipment has been on the increase. 24,25 Hepatitis A and hepatitis B have been stable (though there was an outbreak of hepatitis A in Bristol in 2000), but hepatitis C has been increasing at a serious rate and 80% of hepatitis C cases are IDUs. 24,25 These studies have estimated that around 50% of IDUs have hepatitis C in the London area and 30% outside London. Moreover, the longer a person has been injecting the higher the likelihood of infection, such that 70% are infected by the time they have been injecting for 15 years.
Sexually transmitted infections have also been on the increase, partly because of drug users becoming sex workers to pay for drugs and the sexually disinhibiting effects of some drugs. For example, there was an outbreak of syphilis in Bristol in 1997/98 associated with crack-cocaine and heroin use. 26
Overdoses and mental health problems
Illegal drugs may be the prime means for deliberate self-poisoning or associated with other methods of self-harm or attempted suicide. People with drug problems are also more likely to have associated mental health problems (dual diagnosis) and to self-harm. 27,28
Accidents and injuries
Under the influence of drugs, accidents and injuries are more likely to occur, whether at home, by neglect, e.g. causing fires, or whilst driving or engaged in drug related crime.
Back
Health effects on others
Drug misuse has damaging effects on family members and the wider community. Living with someone with a drug problem can be harrowing and isolating, giving rise to a range of psychological problems. Partners are also more prone to the transmission of infection, and babies born to problem drug users are at risk of neonatal addiction and the intrauterine transmission of infection. Children are vulnerable and at risk of harm through neglect or abuse (see McKeganey, 2001 for review 29 ). There is also evidence of an increased likelihood of later drug misuse, and at a relatively young age. 30
Back
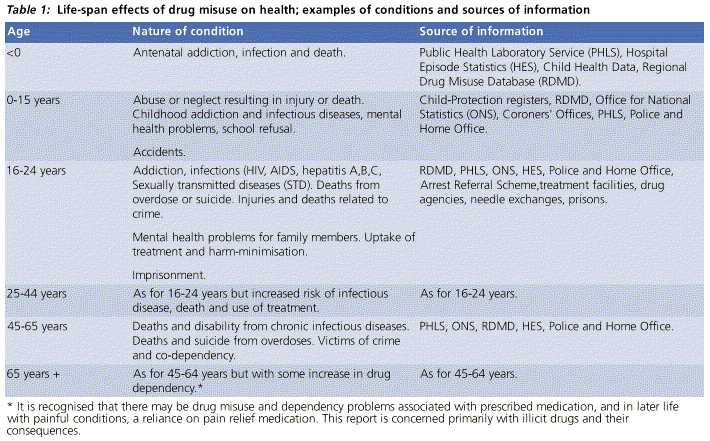
Life span approach
From the above it is clear that drug misuse has far reaching effects, not only on the user but also on families, children and the wider community. It may affect people across the life span. Table 1 shows more clearly the impact of drug misuse on the health of people of different ages.